
More Information
Submitted: October 03, 2023 | Approved: October 16, 2023 | Published: October 17, 2023
How to cite this article: Darroudi A, Abbasi A, Shayestehazar M. Investigation of Malpractice Claims Concerning Orthopedic Surgeons in Sari, North of Iran, 2015-2020. J Forensic Sci Res. 2023; 7: 065-071.
DOI: 10.29328/journal.jfsr.1001052
Copyright License: © 2023 Darroudi A, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Medical malpractice; Orthopedic surgeon; Malpractice claim; Sari; Mazandaran

Investigation of Malpractice Claims Concerning Orthopedic Surgeons in Sari, North of Iran, 2015-2020
Amin Darroudi1* , Ali Abbasi2 and Masoud Shayestehazar3
, Ali Abbasi2 and Masoud Shayestehazar3
1Student Research Committee, Sari Branch, Islamic Azad University, Sari, Iran
2Pathology and Legal Medicine Department, Sari Branch, Islamic Azad University, Sari, Iran
3Orthopedic Research Center, Mazandaran University of Medical Sciences, Sari, Iran
*Address for Correspondence: Amin Darroudi, Student Research Committee, Sari Branch, Islamic Azad University, Sari, Iran, Email: [email protected]
Introduction: Treatment failure and claims against physicians may have many negative consequences. Orthopedic surgeons have always been among the most used specialists. Therefore, the investigation of causes and the process of these claims can help reduce the negative effects of medical malpractice on physicians and society.
Materials and methods: This retrospective study investigated all medical orthopedic negligence cases in Sari, Iran, from March 2015 to March 2020. Data were collected using a researcher-made checklist and analyzed in SPSS software (V-21).
Results: Out of 57 finalized cases investigated in this study, surgeons were found liable in 23 (40%) cases. The mean ± SD age of patients was 41 ± 19.3. Moreover, the level of education had a positive correlation with the surgeon’s liability. The most common cause of complaint was reduced Range of motion (ROM) and the most common type of complained surgery was “open reduction & internal fixation” (ORIF). None of the surgeons were found liable due to surgical site infection or device failure. The mean ± SD time for the file processing was 11.1 ± 10.1 months. The mean indemnity payment was 320 million Iranian Rials (9.7% of indemnity for death in Iran).
Conclusion: The most effective way to reduce medical complaint cases is to increase the knowledge and skill levels of physicians. The lack of a blinded arbitration system in both organizations could lead to bias in the case assessment process. Moreover, considering the long processing time of the claims, it is recommended that new technologies should be used to reduce the time and increase the accuracy of the final verdict. The absence of a ‘no-fault’ compensation program is a significant flaw in Iran violating patients’ rights. Also, more studies are needed to evaluate justice and equality in Iranian medical commissions.
It is not an exaggeration to claim that no person or system is immune from error. The same applies to the field of treatment despite all the advancements in this area [1]. Accordingly, physicians can always expect to be exposed to “medical maltreatment” lawsuits by their dissatisfied patients. Several studies carried out inside and outside the country revealed that the number of complaints against physicians and other healthcare workers has increased despite tangible advances in the methods of diagnosis and treatment in recent years [2,3]. Studies have shown that medical malpractice is the third cause of death in the United States [4]. Consequently, patients’ complaints and dissatisfaction have become one of the critical issues facing the medical professions [5].
However, the judicial investigations proved that the majority of these complaints were baseless and the physicians were acquitted of the allegations [3]. It is worth mentioning that more than 1,500 complaints have been registered against physicians in the Legal Medicine Organization(LMO) of Iran in 2010 [6] apart from those registered and processed in the Medical Council (MC) of Iran which is a parallel professional organization to assess these claims. Additionally, the number of medical malpractice complaints has increased in recent years, as mentioned above.
Surgeons and especially orthopedic specialists have always been at the forefront of the risk of medical complaints. In a study conducted by Dr. Fallah, et al. in Iran, it was found that the probability of a medical malpractice complaint against an orthopedic specialist is four times that of a gynecologist and three times that of a general surgeon or otorhinolaryngologist. Also, the results of a large number of studies revealed that the majority of medical malpractice cases occur by orthopedic specialists [7].
The legal complaint against physicians can have adverse psychological and social impacts, such as permanent impairment of the patient, weakened physician-patient relationship, waste of time, depression in doctors, and the promotion of defensive medicine, along with financial costs to patients, doctors, and legal authorities for investigating the case [8,9]. Accordingly, the identification of high-risk conditions leading to medical complaints as well as the investigation of the cause of complaints by patients with orthopedic problems can be helpful for decision-making in medical and educational systems and training of physicians (especially orthopedic specialists). Moreover, it can prevent the filing of medical complaints and relevant complications and help doctors act more successfully in getting the satisfaction of their patients. The investigation of the voting process of claims in responsible organizations or courts can lead to find pathology of this judicial procedure and achieve fairer handling of the case in relevant judiciaries. Unfortunately, only a few and often outdated original studies have been conducted in Iran on the cases of complaints against physicians. Therefore, there is a need for updated studies in this field [7].
To be clear in Iran, patients have two options to lodge complaints against physicians and healthcare workers and other committees such as hospitals’ mortality committees just investigate cases to improve the quality of services. The first option is to approach the regional MC, which refers the cases to local specialists for their expert opinions. The MC then convenes a board meeting to reach a decision. If either the patient or the healthcare worker disagrees with the decision, the case can be escalated to the MC of the province. In instances where healthcare workers are found liable, they may face professional restrictions or penalties and are required to settle with the patients. If a resolution cannot be reached, the case may be escalated to the court for legal redress. Legal consequences can include compensation for injuries and even imprisonment in severe cases.
Alternatively, patients can directly initiate legal proceedings in court, either initially or following an unsatisfactory outcome from the MC’s decision. In these instances, the court typically refers the case to the LMO to obtain expert opinions. The LMO board consists of at least five experts, including trustworthy doctors specialized in the relevant field and experts in legal medicine. In cases where there is an objection from either the healthcare worker or the patient, the case is referred to the LMO of another province for reevaluation by additional experts. Ultimately, the court makes its decision based on the expert opinions provided by the LMO.
Compensation amounts in Iran are determined according to the national Islamic Indemnity guidelines by the judicial system [10]. Compensation is calculated based on the severity of injury sustained as well as the estimated percentage of fault attributed to the causal malpractice role. For instance, the mortality rate of severe myocardial infarction would still be high despite the proper treatment. Hence, in case of death due to that, the indemnity amount is set at approximately 50% of the maximum payment schedule allotted for wrongful death claims, reflecting the gravity of the injury yet acknowledgment of medical malpractice factors.
National Islamic Indemnity guidelines determined full indemnity for most organs [11] for instance, the indemnity of missing both hands or both eyes are same and equal to death. Therefore, if the injury causes the missing of two hands and one eye the allocated indemnity would be equal to one and a half death indemnity.
There are four types of malpractice in Iran’s judicial system including imprudence, carelessness, lack of skills, and outlawry. Outlawry such as doing something by a non-certified person for that is not covered by physician’s Liability insurance [12].
This retrospective descriptive-analytical study was conducted on the medical complaint cases dated from March 2015 to March 2020. In this study, the necessary permits were initially obtained from the Ethics Committee of Research(approval ID: IR.IAU.SARI.REC.1399.038) [13], MC and LMO of Sari, Iran. Subsequently, all medical malpractice cases that were available in the archives of the aforementioned organizations were reviewed using the census method. A systematic review was conducted in the archives of both organizations and the orthopedics files that have been sent to the relevant commissions within the specified period were extracted (Figure 1). Afterward, the checklists were completed confidentially inside the departments using the data within the extracted files. Subsequently, the data were transferred to Excel software and presented as a code sheet. Data analysis was conducted using SPSS software (version 21).
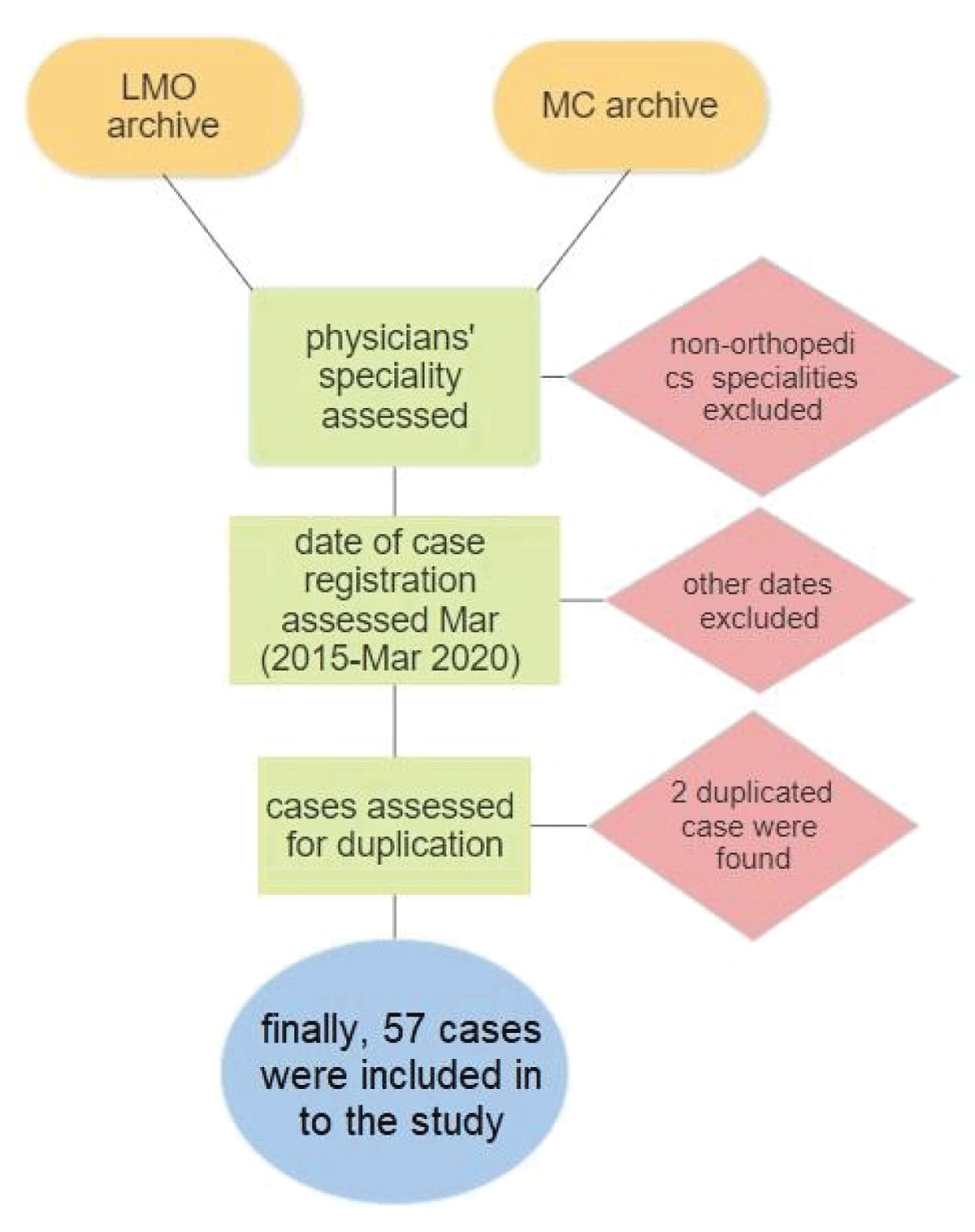
Figure 1: Flowchart of the case selection process.
Out of the total 57 medical complaint cases investigated in this study, 15 and 42 (73.7%) cases were prepared and reviewed by Sari MC and LMO located in Sari, Iran, respectively. The trend of complaint registration has been stable over these five years and there have been no significant changes
(Figure 2). Physician’s malpractice has been confirmed by the final verdict of 23 (40%) cases; however, in 34 cases the doctors have been acquitted from the charge of medical malpractice. The physician’s malpractice has been determined as carelessness, imprudence, and lack of skill in 6 (26%), 6, and 11 cases (47%), respectively.
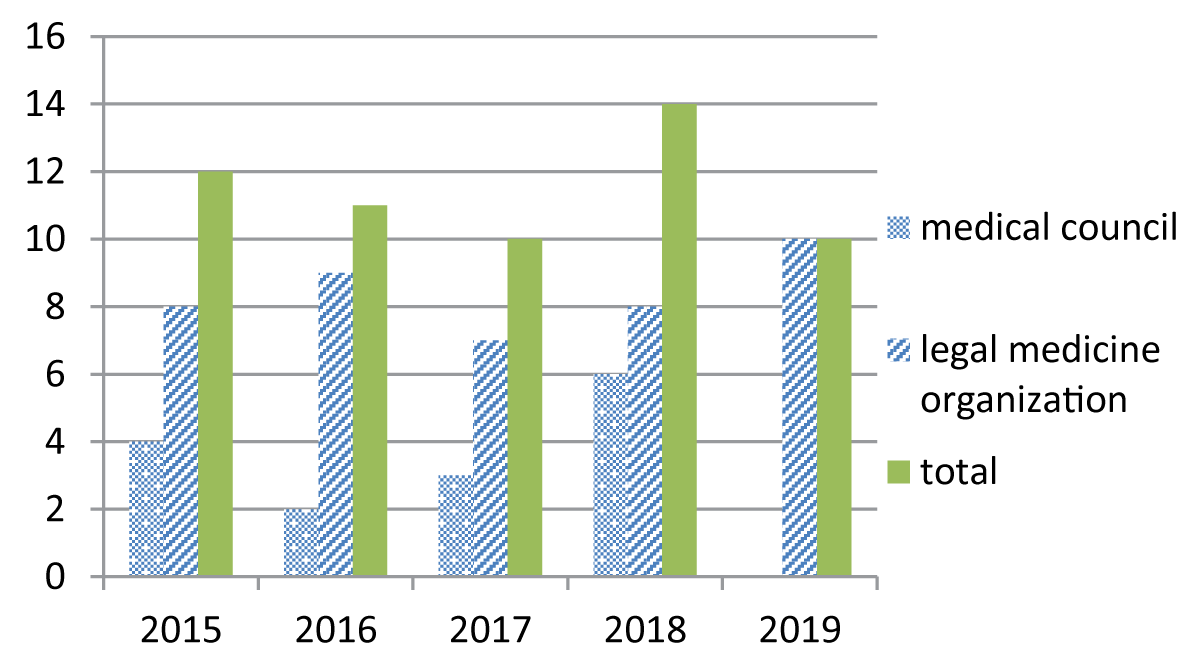
Figure 2: Frequency of complaint files in different years.
The majority (n = 48, 84%) of plaintiffs in this study were male patients. The youngest and oldest patients were a four-year-old boy and a 77-year-old man, respectively. The total mean ± SD age of the patients was 41.2 ± 19.3 years. The mean ± SD age for female and male patients was 51.7 ± 16.47 and 39.7 ± 19. 36. It is worth mentioning that 38 (79%) and 6 (66%) cases of complaints by males and females were due to traumatic injuries, respectively, and other cases of complaints were filed by patients with orthopedic diseases.
The educational information of 51 plaintiffs was available from whom 5 (10%) patients were illiterate and only 8 (16%) patients had a university degree. The highest level of academic education was a master’s degree. Moreover, 21 and 17 patients had unfinished high school education and high school diploma, respectively. It should be noted that in the case of patients under the legal age, the education level of the plaintiff’s guardian was registered. The correlation between patient education and medical malpractice was investigated using the Kendall correlation test. In this regard, the correlation coefficient of -0.26 with a significance level of 0.047 indicated the correlation between these two variables. Therefore, although patients with higher education had declared fewer complaints, they had a higher chance of winning the case. Other demographic characteristics had no relationship with the final verdict.
The complaint cases were analyzed based on the type of treatment center. It was found that the majority of complaints were related to educational centers (n = 23, 40%). (Figure 3).
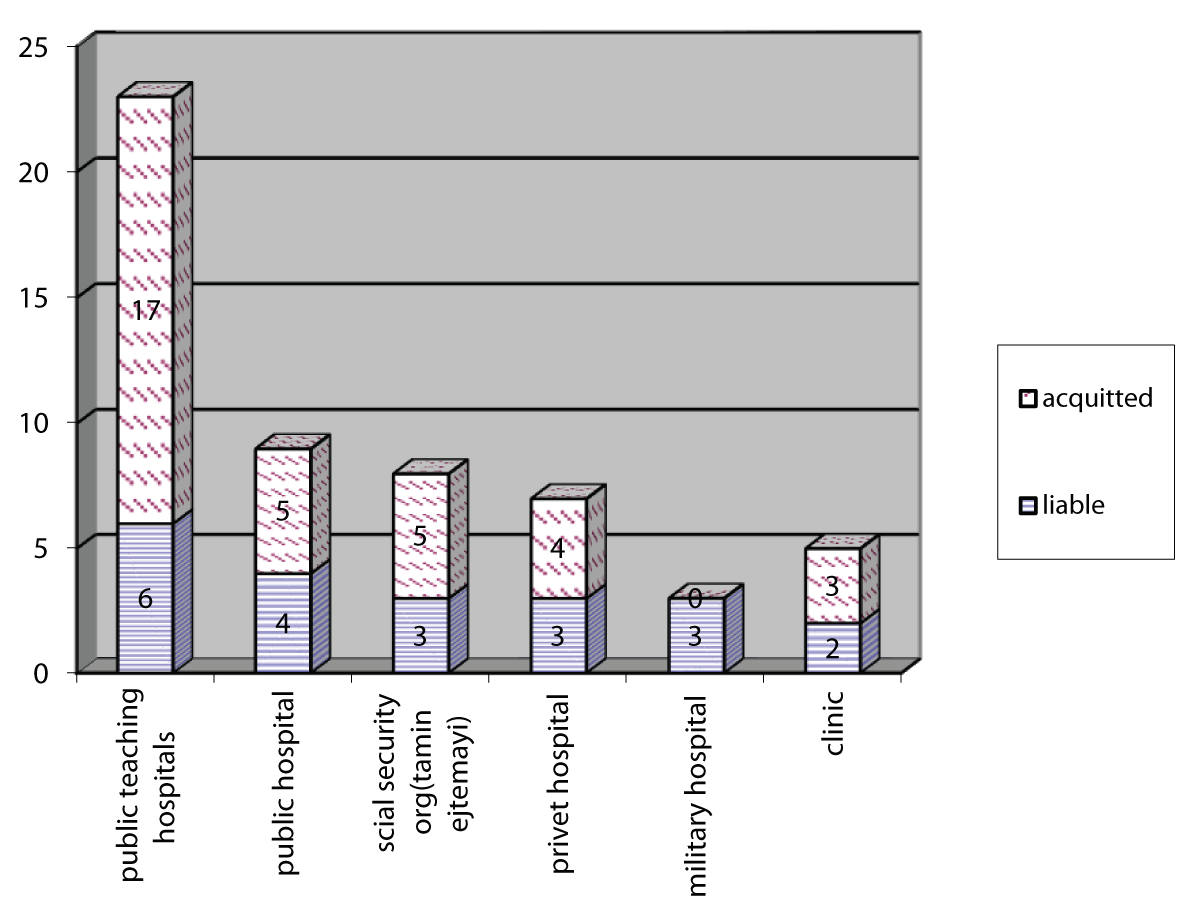
Figure 3: Frequency of various medical centers involved in complaints.
Out of the total 57 complaints, 24 (42%), 31, and 2 cases were related to the upper limbs, lower limbs, and multiple fractures, respectively. The most common organs associated with the complaint were the knee (n = 9), the hand (n = 8), and the leg (n = 7), respectively (Figure 4). Moreover, the most common cause of patients’ complaints included reduced ROM (21%) followed by imposed additional costs on the patient (18%), and infection (14%). (Table 1) It is worth mentioning that some patients have mentioned two or three reasons for their complaints.
| Table 1: Cases divided by cause of complaint. | |||
| Cause of complaint | Final verdict | Total | |
| Medical malpractice | Lack of medical malpractice | ||
| Death | 0 | 2 | 2 |
| Reduced ROM | 9 | 9 | 18 |
| Limb shortage | 2 | 1 | 3 |
| Infection | 4 | 8 | 12 |
| Device failure | 0 | 5 | 5 |
| Nerve damage | 1 | 0 | 1 |
| Malunion | 4 | 4 | 8 |
| Nonunion | 4 | 2 | 6 |
| Chronic pain | 1 | 2 | 3 |
| Misdiagnosis | 1 | 0 | 1 |
| Infliction of additional costs | 11 | 5 | 16 |
| Amputation | 2 | 1 | 3 |
| Necrosis | 1 | 1 | 2 |
| Physician misconduct | 1 | 2 | 3 |
| Others | 2 | 3 | 5 |
| Total | 43 | 45 | 88 |
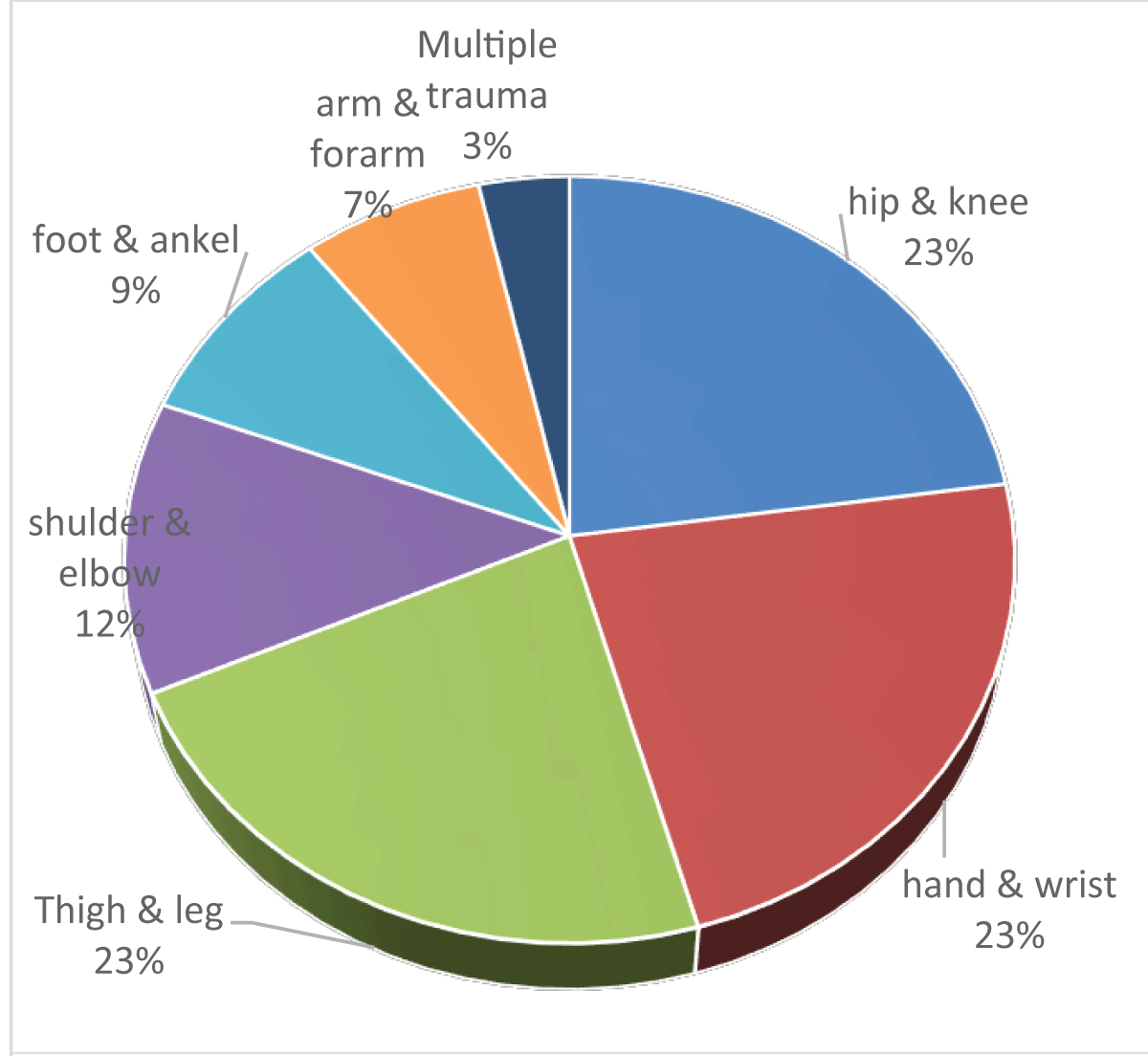
Figure 4: Frequency of organs involved in complaints.
The surgery with the highest number of complaints was “ORIF” (29%), followed by “soft tissue repair” (17%) and “arthroplasty” (15%). (Table 2) The highest failure rate (100%) belonged to arthroscopic surgeries. The highest number of malpractices was related to “ORIF” (n = 9) and “soft tissue repair” (n = 6) surgeries (Table 2). It should be noted that two or three types of surgery were considered for some patients.
| Table 2: Cases divided by type of surgery. | |||
| Surgery type | Final verdict | Total | |
| Medical malpractice | Lack of medical malpractice | ||
| ORIF | 9 | 11 | 20 |
| CRIF | 1 | 6 | 7 |
| Arthroplasty | 5 | 5 | 10 |
| Amputation | 1 | 1 | 2 |
| Soft tissue repair | 6 | 6 | 12 |
| Cast or Splint | 3 | 5 | 8 |
| External fixator/ tension | 0 | 1 | 1 |
| Device removal | 2 | 1 | 3 |
| Osteotomy and deformity correction | 3 | 1 | 7 |
| Arthroscopy | 2 | 0 | 2 |
| Total | 32 | 37 | 69 |
Infection was the cause of the complaint in 12 cases for which the physician was found liable in 4 (33%) cases. This failure rate is slightly lower than the overall failure rate (40%); however, no significant relationship was observed in the analysis (p = -0.07). It should be noted that infection was not the reason for the surgeon’s liability in the mentioned four cases and there were other causes of complaint in these cases as well. Moreover, in these cases, the medical malpractice was considered to be due to a defect in the surgical technique (n = 2), lack of proper follow-up and management of complications (n = 1), or the failure to explain possible complications to the patient when informed consent was received. Additionally, surgical site infection (SSI) has always been mentioned as a probable complication of surgeries which cannot prove any malpractice in the verdicts of the medical commissions.
Out of 16 cases in which the imposed additional cost was considered to be the cause of complaints, 11 cases (69%) led to the doctor’s liability. Statistical analysis indicated that the infliction of additional cost was strongly correlated with medical malpractice (p = 0.006). The doctors were acquitted in all five complaint cases that were filed due to the failure of orthopedic devices. Therefore, the rate of malpractice due to device failure was 0% (correlation coefficient of -0.25). Despite the one-sided results, the small number of samples showed a weak inverse relationship between these two variables (p = 0.05). Other causes of complaints were not associated with medical malpractice (Table 2).
The existing cases were raised in medical commissions from 1 to 4 times due to protests from both sides of the complaint. Voting time analysis was performed on 47 cases in which the time of registering the complaint and the time of the final medical commission’s vote were announced. The minimum and maximum time from the reception of the complaint case to the issuance of the final verdict was 15 days and 54 months, respectively. The mean ± SD of this time was 11.1 ± 10.1 months. In total, 102 medical commissions have been held for these 57 cases of complaint.
The mean ± SD time for voting on each complaint case (the verdict of each commission) was 6.84 ± 6.11 months. The mean ± SD voting time in LMO and MC. was 5.96 ± 4.69 months and 8.25 ± 7.78 months, respectively. Therefore, it can be concluded that on average the verdicts have been issued 69 days sooner in LMO.
The range of MC.No. Of physicians was considered as a criterion for their work experience and its relationship with the final verdict of the medical commission was examined as well. No relationship was observed between the final verdict and the given MC. No. (Work history).
Complaint files were also investigated in terms of the surgery day. Interestingly, the highest number of complaints (n = 10; 25% of the total complaints) and the highest rate of failure (60%) belonged to surgeries performed on Sunday (2nd day of Islamic week). Moreover, five surgery-related complaints were registered on Monday none of which surgeons were considered liable. Therefore, Monday was the weekday with the lowest failure rate (0%). However, statistical analysis showed no significant relationship between the day of surgery and surgeon’s liability which can be due to the small number of samples. It should be noted that, the exact date of the operation was not available in some cases or that the complaint could not be related to a specific operation for various reasons, including multiple surgeries.
In total, the indemnity payment was determined for 22 patients. The minimum and the maximum indemnity payment equaled 1.2% and 33% of the indemnity for death. The mean ± SD rate of indemnity payment determined was 9.7% ± 8.8%. The indemnity of death was 3.3 billion Iranian rials in 2020(20 thousand USD). Therefore, the liable surgeons have paid an average of 320,010,000 ± 290,304,000 Rials as compensation to their patients.
Based on the obtained results, no statistically significant increase or decrease was observed in the general trend of complaint registration in the investigated five years. Although this trend has been increasing in the world over the past decades, studies conducted inside the country have shown contradictory results regarding the trend of medical complaint registration in recent years.
In the same line, Kalani, et al. in a systematic review showed just a slightly decreasing trend in registering claims against physicians [14]. The result of the study performed by Siabani, et al. which was not included in Kalani’s study, indicated that the number of registered complaints in Kermanshah, Iran, increased between 2001 and 2005 [15]. Although the MC and LMO of Iran have not provided official statistics on the number of registered complaints, it seems that a balance has been reached in terms of the number of registered cases and that the number of complaints has been relatively constant in recent years.
On the other hand, the prevalence of social networks and the improvement of trade union relations has led to an increase in the spread of bad news related to medical malpractice in recent years, which can, in turn, reduce the number of complaints and medical malpractice by raising doctors’ awareness. However, sometimes the spread of rumors, exaggeration, and bad news regarding the increase in medical complaints can overshadow the doctor-patient relationship in a negative way [16].
However, it should be noted that the fear of complaints from unsatisfied patients is the most common cause of defensive medicine behavior among physicians [17] and can impose huge costs on patients and medical systems [18]. Therefore, regarding the high prevalence of defensive medicine in Iran [9], the relevant authorities, including the MC of Iran, the Ministry of Health, as well as LMO need to create awareness among doctors and follow practical solutions such as advancing the insurance system. This way they not only can raise the number of successful treatment cases and improve the physician-patient relationship but can also reduce the anxiety of physicians and prevent the infliction of huge unnecessary costs on the country [19].
In this study, the majority (84%) of plaintiffs were male, which was consistent with other studies results of other studies on orthopedic malpractice [20], since 77% of causes of orthopedic complaints were due to trauma and males were more likely to experience trauma. In the same line, the results of a study carried out by Sonmez indicated that 20% of medical complaints were related to occupational accidents, to which males are naturally more exposed [21]. Moreover, based on the published statistics, males are more likely to be involved in traffic accidents [22].
The education level of 51% of the plaintiffs in this study was below the high school diploma. At the same time, the result of the national census in 2016 showed that 49% of the over 20-year-old population in this province (Mazandaran) have below diploma education [23], showing our study’s sample is homogenous in this variable. It was shown that people with lower education levels were less likely to prove medical malpractice, which is a serious alarm for systematic inequality. Unfortunately, in previous similar studies, the association between education level and Medical Commission verdict was not examined; however, this finding can be considered from two perspectives. From one perspective, there is a doubt that educated people are not treated fairly in medical commissions; however, from another perspective, there is a probability that the rate of baseless complaints is higher among these people for various reasons. For example, physicians may not spend enough time explaining the conditions and complications of the disease to these patients, or they may mistreat them and provoke them to file a complaint. Moreover, these patients may be attributed to the fact that due to their poor economic condition, these people have a higher tendency to seek compensation in any way possible. However, detailed studies on the relation between the education level of plaintiffs and the final verdict as well as the motivation of these patients for filing a complaint seem to be necessary. Therefore, physicians need to know that this group is prone to filing unnecessary complaints and that they should be more cautious to prevent lawsuits during the treatment process.
Based on the evidence, medical commissions acquit physicians from the charge of medical malpractice in cases where injury has been caused by SSI or the failure of the used devices and consider these as natural complications of surgeries. However, many studies in other countries have shown that doctors were considered guilty of medical malpractice and were required to pay a penalty for SSI or a no-fault compensation program to take responsibility to compensate for these injuries [24].
One study revealed that medical negligence has been considered to be the cause of SSI in one-third of complaints following hip arthroplasty [25]. In another study, SSI was considered to be the cause for half of the complaints against orthopedic specialists, and the doctors had to pay an average of 114,000 Euros as compensation for malpractice accordingly, which was the highest amount of compensation fee among the various causes of the complaint [3]. Therefore, the high disparity between the legal authorities in Iran and developed countries on this matter requires serious investigation.
As mentioned before, the average time it took for investigating medical malpractice cases to reach an outcome was 11 months. This number reflects the time spent on issuing final verdicts and is not related to other administrative matters; therefore, the time from filing a complaint to reaching the final result would be longer. Recently, the outbreak of the COVID-19 virus has accelerated the process of remote working in many activities, and remote or online meetings are turning into a routine even in legal matters.
Nowadays, the Iranian LMO is holding online medical commissions in some provinces of the country in a limited way. Therefore, it is suggested that such organizations, especially the MC of Iran, which has a lengthy process for pursuing such legal cases, use online and remote systems extensively and comprehensively. Another advantage of these remote systems is their potential to gather specialists from all over the country simultaneously. Therefore, it is possible to benefit from the most experienced experts in the fastest possible time.
Conflict of interest and unconscious bias are some of the problems of local commissions since especially in small towns, doctors have a lot of personal relationships with each other which might affect their expert opinions. In addition, in several cases, it was observed that the role of physicians had shifted from one of the parties involved in the case to the expert and from the expert to one of the parties. This challenge also could be mitigated by online blinded commissions by a national network of experts.
Regarding the fact that establishing a mechanism to prevent conflicts of interest in the judiciary system has always been recommended [26]; the adoption of an integrated system can reduce conflict of interest to a great extent by referring to several experts across the country. It is also suggested that medical records in this system should be provided without revealing the doctor’s identity so that the commissions are not affected by the reputation or position of the relevant doctor. This can highly minimize bias and preserve the confidentiality of documents.
Baes on the obtained results in the present study, doctors were acquitted in 60% of complaint cases. However, since some cases were referred from other provinces or several cases were omitted in the medical system of other cities and were referred to the LMO of Sari, Iran, only to determine the amount of indemnity payment, it seems that the real rate of complaints leading to doctors’ liability was about ten percent less (i.e., about 30%) than what has been obtained in the present study. Therefore, the results of this study indicate that most of the medical negligence complaints are ineffective, which is consistent with most of the studies conducted inside and outside the country, such as those carried out by Agout [3], Sadr [1] and Raeissi [4].
It is shown the same as other studies in Iran most of the negligence cases were imprudence type.
Although LMO has provided some technological interventions in their process due to COVID pandemic limitations, the decision process especially in MC is still slow and potent for various biases. Therefore, serious interventions are also needed to improve this process.
Unfortunately, in no-fault injuries such as device failure and SSI, no one compensates that in Iran. Hence, intervention to start some foundation for this flaw seems necessary for the Iranian medico-legal system.
The authors have no relevant financial or non-financial interests to disclose. They would like to thank the esteemed staff of the LMO and MC of Sari, Iran, for their assistance and cooperation during this study.
- Sadr SS, Ghadyani MH, Bagher Zadeh AA. Assessment of records of complaints from medical malpractice in the field of orthopedic, in the coroner’s Office of Forensic Medicine, province of Tehran, during 1988 to 2003. Scientific Journal of Forensic Medicine. 2007; 13(2):78-86 .
- Khammarnia M, Kavosi Z, Ghanbari JM, Moradi A. Impact of clinical governance on patients’compliance in shiraz public hospitals. 2016 .
- Agout C, Rosset P, Druon J, Brilhault J, Favard L. Epidemiology of malpractice claims in the orthopedic and trauma surgery department of a French teaching hospital: A 10-year retrospective study. Orthop Traumatol Surg Res. 2018 Feb;104(1):11-15. doi: 10.1016/j.otsr.2017.11.007. Epub 2017 Dec 13. PMID: 29247818.
- Raeissi P, Taheri Mirghaed M, Sepehrian R, Afshari M, Rajabi MR. Medical malpractice in Iran: A systematic review. Med J Islam Repub Iran. 2019 Oct 14;33:110. doi: 10.34171/mjiri.33.110. PMID: 31934570; PMCID: PMC6946923.
- Haghshenas MR, Vahidshahi K, Amiri A, Rezaee M, Rahmani N, Pourhossen M. Study the frequency of malpractice lawsuits referred to forensic medicine department and medical council, Sari, 2006-2011. Journal of Mazandaran University of Medical Sciences. 2012; 21(86):253-60 .
- Barzgar Bafrouee A, Zarenezhad M, Gholamzadeh S, Hosseini SMV, Gholi A, Gharedaghi J. Evaluation of orthopedic specialists’ malpractice complaints referred to Legal Medicine Organization from 2008 to 2010. Scientific Journal of Forensic Medicine. 2016; 22(1):55-66 .
- Fallah Karkan M, Badsar A, Amir Maafi A, Heydarzadeh A, Rahbar Taramsari M. Survey on malpractice claims against physicians judged in guilan medical council. Journal of Guilan University of Medical Sciences. 2014; 23(91):8-15 .
- Kazemi S, Riahi ME. Individual and Social Impacts of Medical Malpractice Complaints on doctors: A qualitative study. Community Health (SALĀMAT-I IJTIMĀĪ). 2018; 5(2):2018 .
- Daneshkohan A, Ashtar-Nakhaei F, Zali A, Kakemam E, Zarei E. Defensive medicine and its related risk factors: evidence from a sample of Iranian surgeons. Hosp Pract (1995). 2023 Apr;51(2):101-106. doi: 10.1080/21548331.2023.2189370. Epub 2023 Mar 10. PMID: 36882330.
- Ghorbani M, Ghodoosi AJIJoFM. The survey of manner of determining amounts of blood money in brain death injuries from the judges and coroner physicians Viewpoint. 2012; 18(2):107-12 .
- Hossein Alizadeh A, Sadeq Musavi SM, Kousha AJMLJ. Comparison of Calculation of Disease Burden Based on DALY Index and How to Calculate Blood Money Payment. 2018; 1 2(45):29-58..
- Abbasi MMH, Amyan A, Safari S, Tahghighi MM, Robati FK, Langari AA. Medical Malpractice Cases in Kerman Province, Iran (2010-2014). 2020; 24 (2).
- Committees RE. Research Ethics Committees Certificate 2020. https ://ethics.research.ac.ir/ProposalCertificateEn.php?id=137001&Print=true&NoPrintHeader=true&NoPrintFooter=true&NoPrintPageBorder=true&LetterPrint=true .
- Kalani N, Hatami N, Zarenezhad M, Doroudchi A, Foroughian M, Raeyat Doost ER. A systematic review and meta-analysis of medical malpractice studies in Iran. 2021; 79(5):375-83 .
- Siabani S, Alipour AA, Siabani H, Rezaei M, Daniali S. A survey of complaints against physicians reviewed at Kermanshah Medical Council 2001-2005. J Kermanshah Univ Med Sci. 2009; 13(1):74-83 .
- Al-Balushi AA. In the Era of Social Media: Is it time to establish a code of online ethical conduct for healthcare professionals? Sultan Qaboos Univ Med J. 2020 Feb;20(1):e25-e28. doi: 10.18295/squmj.2020.20.01.004. Epub 2020 Mar 9. PMID: 32190366; PMCID: PMC7065697.
- Zarei E, Ashtar-Nakhaei F, Daneshkohan A, Zali A. The first survey on defensive medicine among Iranian surgeons: prevalence and its related factors. 2019 .
- Panella M, Rinaldi C, Leigheb F, Knesse S, Donnarumma C, Kul S, Vanhaecht K, Di Stanislao F. Prevalence and costs of defensive medicine: a national survey of Italian physicians. J Health Serv Res Policy. 2017 Oct;22(4):211-217. doi: 10.1177/1355819617707224. Epub 2017 May 23. PMID: 28534429.
- Rezayi A, Vafaee Najar A, Houshmand E, Esmaeli H, Kouhestani S. Experience and etiology of defensive medicine in view of residents in Mashhad University of Medical Sciences in 2016. Journal of Paramedical Sciences & Rehabilitation. 2017; 6(2):60-8 .
- Lv H, Li D, Li C, Yuwen P, Hou Z, Chen W, Zhang Y. Characteristics of the medical malpractice cases against orthopedists in China between 2016 and 2017. PLoS One. 2021 May 12;16(5):e0248052. doi: 10.1371/journal.pone.0248052. PMID: 33979345; PMCID: PMC8115811.
- Sönmez MM, Seçkin FM, Sen B, Birgen N, Ertan A, Oztürk I. Adli Tip Kurumu'ndan görüş sorulan ve ortopedi uzmanlik alanina giren tibbi uygulama hatalarinin gözden geçirilmesi [A review of malpractice claims concerning orthopedic applications submitted to the Council of Forensic Medicine]. Acta Orthop Traumatol Turc. 2009 Aug-Oct;43(4):351-8. Turkish. doi: 10.3944/AOTT.2009.351. PMID: 19809233.
- Saberian P, Farhoud AR, Hasani-Sharamin P, Moghaddami M, Keshvari F. Epidemiological Features of Injured Patients Examined by Tehran Emergency Medical Service Technicians. Adv J Emerg Med. 2019 Jun 25;3(4):e40. doi: 10.22114/ajem.v0i0.198. PMID: 31633095; PMCID: PMC6789067.
- Iran SCo. 2016 [Available from: https://www.amar.org.ir/english/Population-and-Housing-Censuses/Census-2016-Detailed-Results .
- Howard A, McWilliams T, Hannant G, Saghir N, Giannoudis P, Scott J. Could no-fault compensation for medical errors improve care and reduce costs? Br J Hosp Med (Lond). 2019 Jul 2;80(7):387-390. doi: 10.12968/hmed.2019.80.7.387. PMID: 31283388.
- Zengerink I, Reijman M, Mathijssen NM, Eikens-Jansen MP, Bos PK. Hip Arthroplasty Malpractice Claims in the Netherlands: Closed Claim Study 2000-2012. J Arthroplasty. 2016 Sep;31(9):1890-1893.e4. doi: 10.1016/j.arth.2016.02.055. Epub 2016 Mar 9. PMID: 27062353.
- Pashaee H, Motamedi J. The Judicial Processes Correction in The Light of the Strategy of Elimination of Conflict of Interest. Private Law. 2019; 16(1):67-88.