
More Information
Submitted: September 19, 2022 | Approved: September 22, 2022 | Published: September 23, 2022
How to cite this article: Kearse KP. Ultraviolet fluorescent detection of elevated bilirubin in dried blood serum. J Forensic Sci Res. 2022; 6: 049-052.
DOI: 10.29328/journal.jfsr.1001036
Copyright License: © 2022 Kearse KP. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.

Ultraviolet fluorescent detection of elevated bilirubin in dried blood serum
Kelly P Kearse*
Knoxville Catholic High School, 9245 Fox Lonas Road, Knoxville, TN, 37922, USA
*Address for Correspondence: Kelly P Kearse, Knoxville Catholic High School, 9245 Fox Lonas Road, Knoxville, TN, 37922, USA, Email: [email protected]
Increased levels of bilirubin in blood serum may result from numerous physical conditions including hepatitis, cirrhosis, enzyme deficiency, drug reactions, autoimmune disorders and physiological trauma. No presumptive test for high bilirubin levels in blood serum stains currently exists, which could prove useful in the assessment of crime scenes involving victims with one of the above disorders. Here, the use of ultraviolet 365 (UV 365) is described as a simple, nondestructive method for the detection of blood serum containing elevated levels of bilirubin.
Bilirubin is a product of red blood cell degradation in the liver and under normal conditions, is derivatized to a water-soluble form termed conjugated bilirubin, which is efficiently excreted from the body [1-4]. Total bilirubin measurements of blood serum reflect both the amount of conjugated and unconjugated bilirubin, which in healthy individuals are ~0.6-1.0 mg/dL total, consisting of ~30% conjugated (direct) and ~70% unconjugated (indirect) forms. The unconjugated form of bilirubin is associated with the normal destruction of senescent red blood cells [5,6]. Readings above 3 mg/dL (total) are indicative of some type of health issue, which may involve either unconjugated or conjugated bilirubin forms [5-14]. A relatively high percentage of neonates develop jaundice due to elevated bilirubin levels, which in many cases resolves itself as liver function matures during early life. Medical intervention is necessary if bilirubin levels are greater than 20-25 mg/dL, which if untreated, may result in brain damage and eventually death [3,5]. In adults, increased serum bilirubin levels may result from a variety of conditions including autoimmune disease, cirrhosis, blunt force trauma to the abdomen (liver), hepatitis and hepatocellular disease, where bilirubin levels may reach as high as 20 mg/dL or greater [6-14].
Recently, ultraviolet 365 (UV 365) has been described as an effective alternative light source (ALS) in the detection of blood serum that has dried on various materials [15,16]. This method is useful in evaluating clotting blood that has been transferred as well as an isolated serum that may be cast off, especially in cases where the victim is moved. During previous studies [17], it was noted that the serum halos of clotting blood transfers containing excessive amounts of bilirubin appeared visually different from those of normal, control samples (K.P. Kearse, unpublished observations). It was therefore hypothesized that alternative light sources, specifically UV 365, might be effective in distinguishing serum stains containing elevated levels of bilirubin. Additionally, it was proposed that bilirubin in dried serum stains would be sensitive to photodegradation, similar to circulating bilirubin in vivo and bilirubin in liquid serum samples. Here, the fluorescent detection of blood serum containing elevated levels of bilirubin was evaluated, demonstrating that as bilirubin levels increased, the serum fluorescence shifted from a whitish appearance to greenish/yellow hue. This effect was observed in both dried blood drops and isolated serum. Bilirubin fluorescence was diminished by sun exposure, documenting that bilirubin remains photosensitive in dried serum stains. The implications of these findings in forensic blood detection and analysis are discussed.
Blood and serum
Human blood was obtained from healthy volunteers by the finger stick method using a Health Lancing device (CVS pharmacy, USA) fitted with a micro lancet (CVS Pharmacy, USA). Blood was dropped onto Parafilm® M Laboratory Film (Bemis Company, Inc., Oshkosh, WI) and transferred to various substances using a 1-10 or 10-100 microliter (µl) Eppendorf® micro pipettor (Hamburg, Germany). Human blood serum was obtained from Innovative Research (Innovative Research Company, Novi, MI), purchased as pooled human serum of the clot, and transferred to various substances using a 1-10 or 10-100 microliter (µl) Eppendorf® micro pipettor (Hamburg, Germany).
Bilirubin preparation
Unconjugated and conjugated bilirubin (Lee Biosciences, Maryland Heights, MO) were resuspended in DMSO or water, respectively, at a concentration of 5 mg/ml. Control samples received a solvent amount equivalent to the upper limit used in the experiment. For studies with whole blood and isolated serum, the total endogenous bilirubin level was 0.6 mg/dL and 0.2 mg/dL, respectively.
Ultraviolet light sources
Two UV light systems were used in these studies: a LED UV flashlight, 365 nm, LED-UV301-356 nm (Shenzhen Light Light Limited, Shenzhen, China), referred to as System 1; and two LED portable 3-watt UV light bulbs, 365 nm, UV-3W-365UV-E27-AC (Golden Gadgets, South El Monte, CA) positioned at a ~ 45o angle from the subject and fitted with a NUV M55.0 x 0.75 filters (Edmunds Optics, Barrington, NJ), referred to as System 2.
All photographs were taken using a Sony RX100 digital camera; with System 2, a 425 nm long pass filter (Edmunds Optics, Barrington, NJ) was placed in front of the camera lens.
Fabrics and other materials
Specific fabrics that were used in this study include Whatman® 1 mm filter paper; commercial linens purchased from Joanne’s fabric shop, designated types 1 and 3; natural unprocessed linen (chemical free, unbleached, undyed) made from 100% organically grown flax, designated as type 2; linen that was hand woven from natural, unprocessed flax, designated as type 4; and a white cotton T-shirt that had been worn and washed in commercial detergent for several years. All fabrics were obtained from the author’s personal collection. Other materials include pre-cleaned glass microscope slides, stainless steel kitchen knives, black disposable nitrile gloves, a Ziploc plastic bag and a white leather walking shoe.
Sunlight exposure
Approximately 10 ml of serum containing normal or elevated amounts of bilirubin (10 mg/dL) were added to filter paper and dried. One-half of the sample was exposed to four hours of sunlight on a clear day (~80 oF, relative humidity ~ 60%); the other half was covered and placed alongside the experimental sample. Samples were rejoined for photographic analysis.
As shown in Figure 1, serum containing increasing amounts of bilirubin showed a shift in UV fluorescence from a whitish appearance to a greenish/yellow tinge (Figure 1).
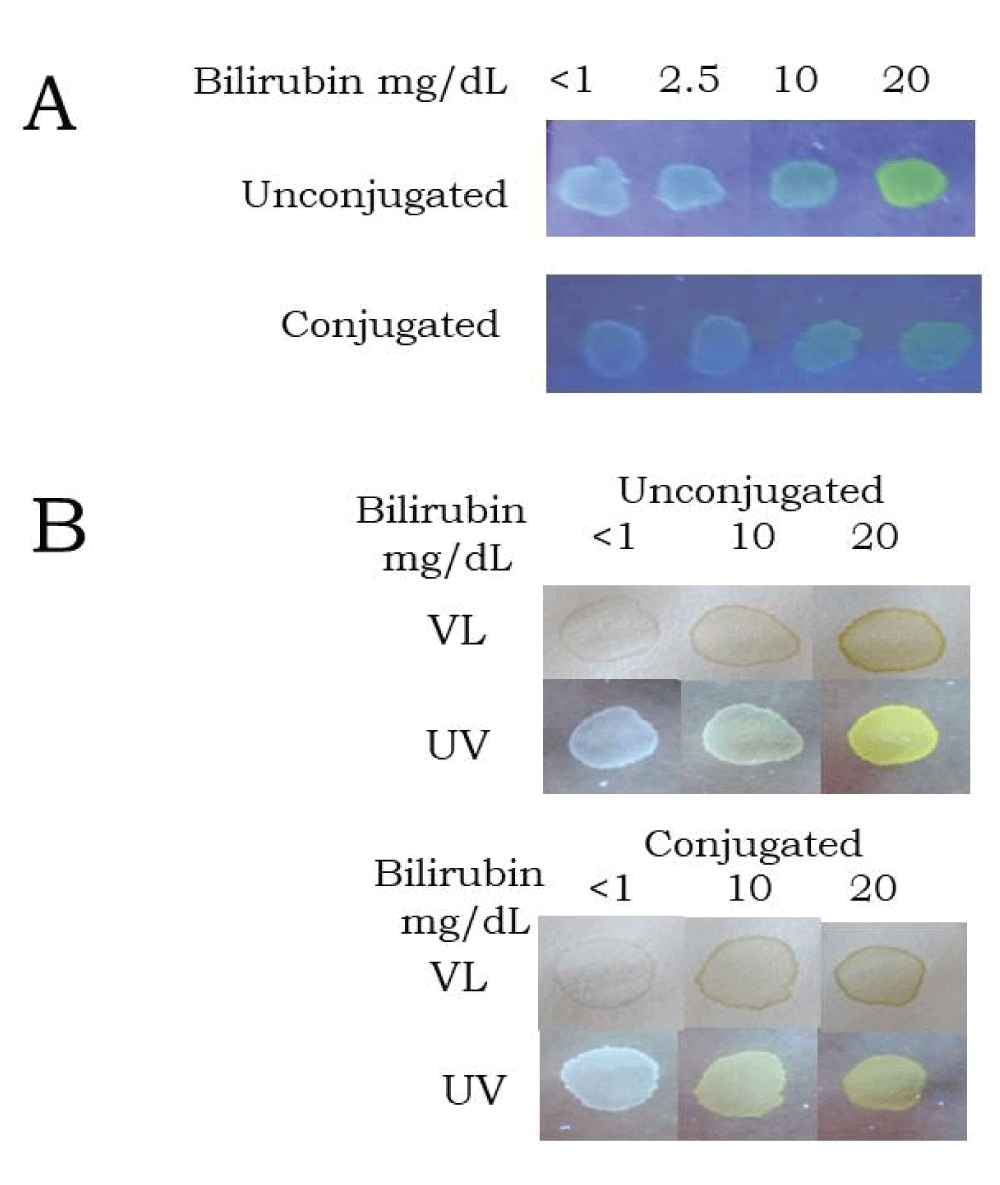
Figure 1: The appearance of control and elevated bilirubin serums under visible light (VL) and UV365. Samples were added to filter paper and evaluated under visible (normal) light and UV 365 using system 1 in (A) and system 2 in (B). See Materials and Methods for details.
This effect was observed using two different UV lighting systems, a portable UV flashlight ideal for field work (Figure 1A) and two LED UV light bulbs fitted with a restrictive filter (Figure 1B), (see Materials & Methods for details). The color shift was observed for both bilirubin forms and was readily distinguished from control serum at concentrations of 10 mg/dL or greater (Figure 1). At relatively high levels (20 mg/dL), serum fluorescence of the unconjugated form was a particularly bright greenish/yellow (Figures 1A & 1B). Blood drops containing normal and elevated levels of bilirubin that had dried on glass or a metal knife blade appeared relatively similar under visible light (Figure 2); however, they were markedly different when examined under UV 365 (Figure 2).
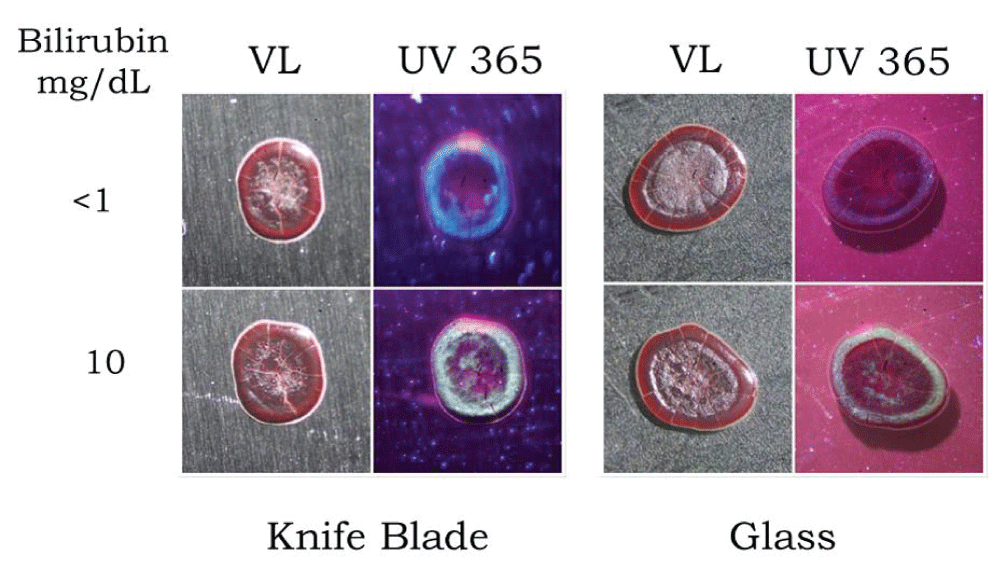
Figure 2: Effect of elevated bilirubin on the appearance of dried blood under visible light (VL) and UV 365. Control and elevated levels of unconjugated bilirubin (10 mg/dL) samples were added to a metal knife blade or glass slide and after drying, evaluated under a stereomicroscope using visible (normal) light or UV 365 (system 1).
In control blood groups, the serum formed a whitish fluorescent ring at the outer edge of the drop, whereas groups containing elevated levels of bilirubin showed a greenish/yellow fluorescent ring at the periphery (Figure 2). Isolated blood serum containing high bilirubin levels that had dried on a metal knife blade was distinguishable from control serum even under visible light, although this difference was clearly enhanced under UV 365 (Figure 3). Similar results were observed with a blood serum that had dried on glass (Figure 4).
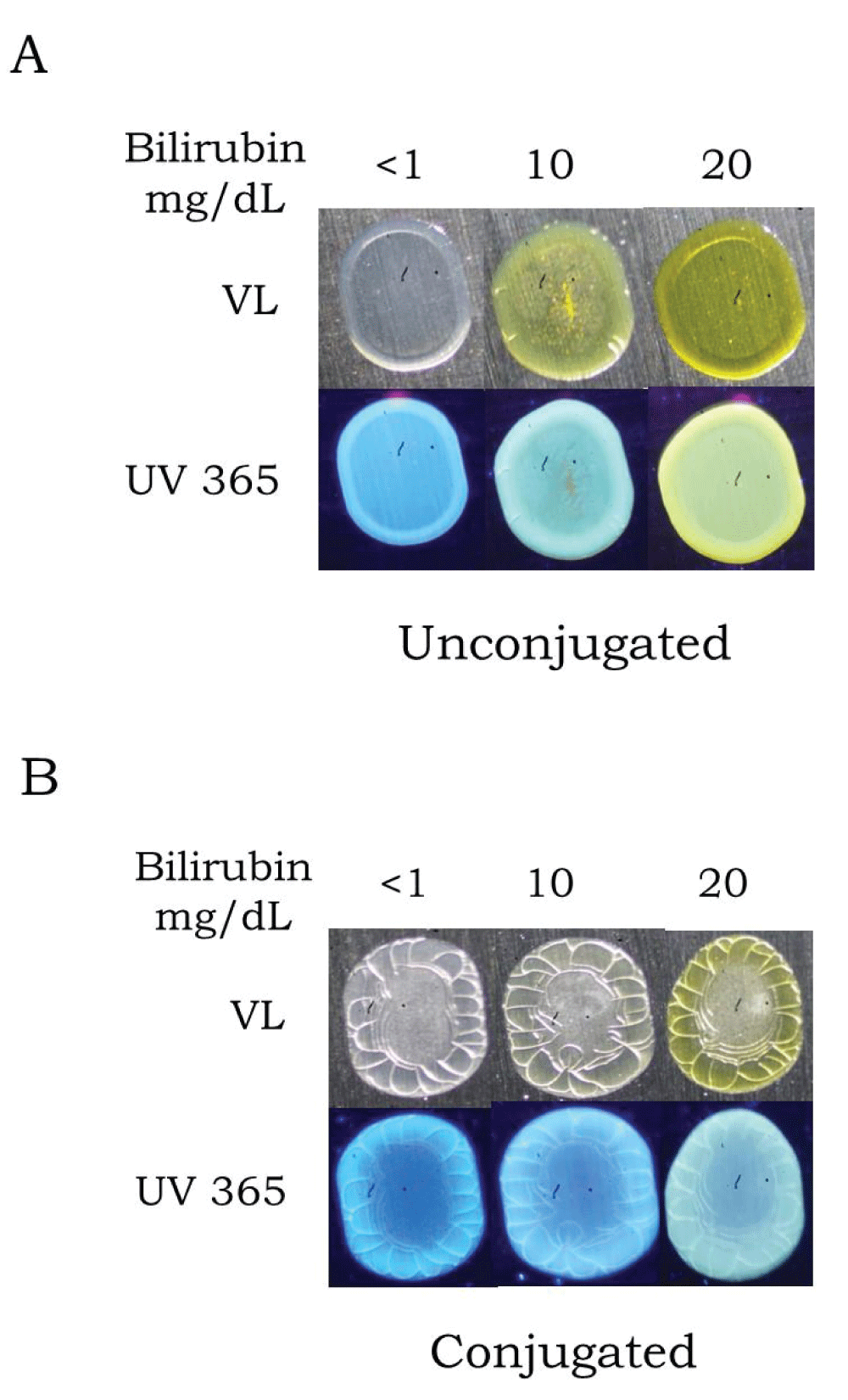
Figure 3: The appearance of serum containing elevated levels of unconjugated or conjugated bilirubin on a metal knife blade. Samples containing increasing amounts of unconjugated (A) or conjugated (B) bilirubin were added to a metal knife blade and after drying, evaluated under a stereomicroscope using visible (normal) light or UV 365 (system 1).
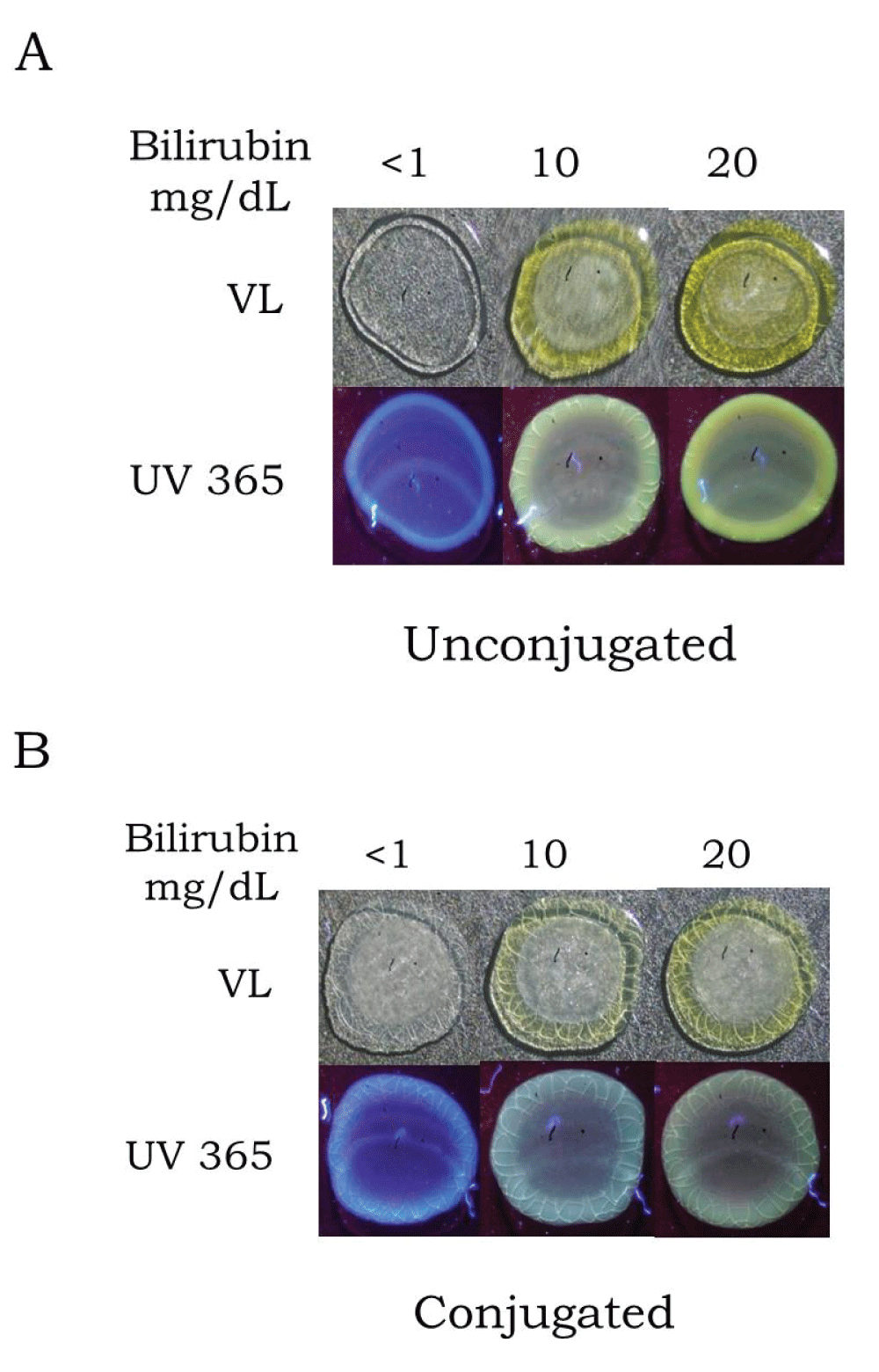
Figure 4: The appearance of serum containing elevated levels of unconjugated or conjugated bilirubin on glass. Samples containing increasing amounts of unconjugated (A) or conjugated (B) bilirubin were added to glass microscope slides and after drying, evaluated under a stereomicroscope using visible (normal) light or UV 365 (system 1).
Detection of serum containing normal and elevated levels of bilirubin on certain textiles and materials was variable, depending on the type of substance examined. Normal serum and elevated bilirubin samples were easily distinguished from each other on nitrile gloves and a plastic Ziploc bag (Figure 5A). With certain linens, control serum was somewhat difficult to detect under UV 365, whereas serum with elevated bilirubin was readily detectable (Figure 5B, Type 1). For other linens, both control and elevated bilirubin serum samples were difficult to visualize (Figures 5B and 5C, Types 2 and 4, respectively), as were serum samples on white cotton (Figure 5D). In contrast, the whitish fluorescence of normal serum and shift to greenish/yellow fluorescence with increased bilirubin were easily visible on Type 3 linen and a white leather walking shoe (Figures 5C and 5D, respectively).
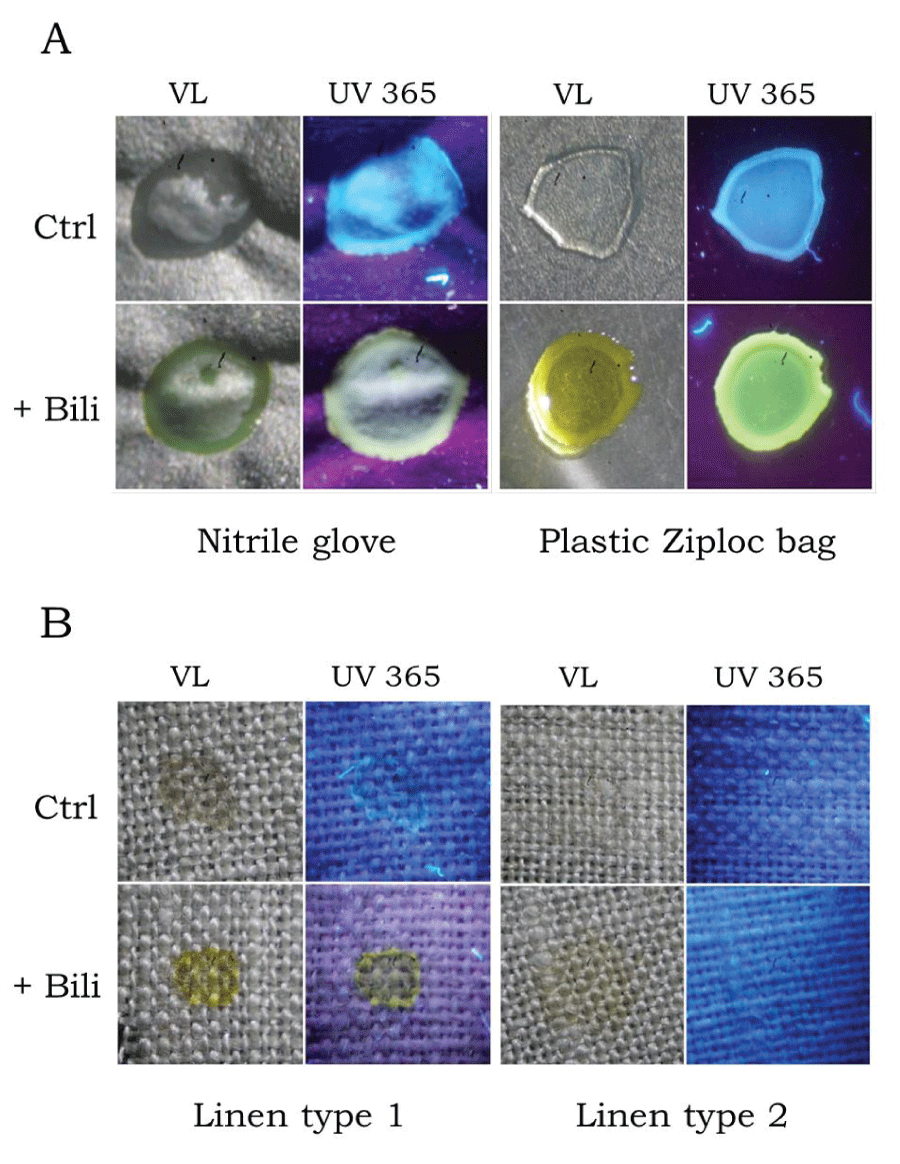
Figure 5: Detection of serum containing elevated levels of bilirubin on various objects. Approximately 5 µL of serum containing normal (Control, Ctrl) or elevated amounts of unconjugated bilirubin (10 mg/dL), (+ Bili), were added to various articles and after drying, evaluated under a stereomicroscope using visible light (VL) or UV 365 (system 1).
Finally, the effect of sunlight exposure on the detection of elevated bilirubin in serum was evaluated. For these studies, control and high bilirubin serums that had dried onto filter paper were cut in half; one half was exposed to sunlight and the other half was covered and placed alongside the experimental group. As demonstrated, the UV visualization of bilirubin was markedly reduced following even a relatively short exposure to natural light, for only four hours (Figure 6).
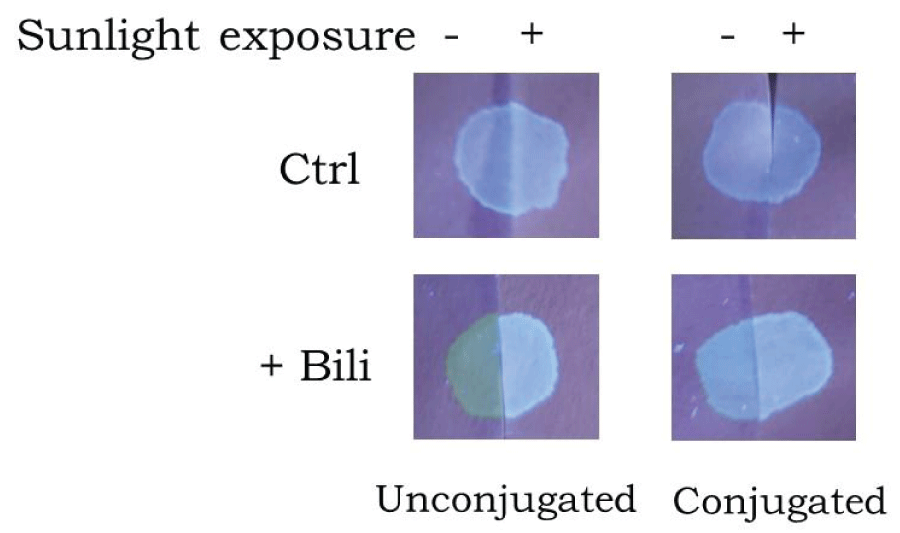
Figure 6: Effect of sunlight exposure on bilirubin UV fluorescence. Serum containing normal (Control, Ctrl) or elevated amounts of unconjugated or conjugated bilirubin (10 mg/dL) was added to filter paper and dried. Samples were cut in half, with one half exposed to direct sunlight for ~ 4 hours; the other half was covered and placed next to the experimental group. For photography, samples were placed alongside each other and evaluated under UV 365 (system 1).
These data document that bilirubin in dried serum stains is light-sensitive, similar to what has been established for bilirubin circulating in (whole) blood [1,3].
The current study has evaluated the identification of dried blood serum containing elevated levels of bilirubin using both visible light and UV 365. The hypothesis that alternative light sources (UV 365) are effective in distinguishing serum stains containing enhanced levels of bilirubin was verified. This analysis may be useful in the initial evaluation of a crime scene where the victim is known or suspected to have a condition resulting in elevated bilirubin levels. As demonstrated, serum with elevated bilirubin was apparent on certain materials even under visible light, having a greenish/yellow appearance relative to normal serum. This is significant as dried blood serum on many substrates is relatively invisible under visible light [15,16]. For some materials, such as certain linens and white cotton, detection of blood serum with UV 365 was difficult, due to a high fluorescent background of the textile onto which the serum had dried. Although UV fluorescence was not particularly useful with serum detection on white cotton, the greenish/yellow tint of elevated bilirubin was apparent even under visible light. For other materials, including certain fabrics, nitrile gloves, and plastic Ziploc bags, control serum was effectively visualized with UV and elevated bilirubin was readily distinguished by increased greenish/yellow fluorescence. Similarly, dried blood droplets from both groups looked relatively similar under visible light but showed distinct differences under UV. If dried blood or cast-off serum containing elevated bilirubin were found on the belongings of a suspect, for example inside of a vehicle (carpet, dashboard, interior trunk latch) and the victim was known to suffer from liver failure or had undergone severe physical trauma, it would be more difficult to explain away as the suspect’s own, if the suspect’s bilirubin levels were normal. As shown in these studies, even very small volumes of blood or serum (5 µL - 10 µL) can be effectively and non-destructively detected using this method. Confirmation that serum was indeed present would, of course, require further testing, similar to evaluation for the presence of semen or saliva. The bilirubin levels used in these studies fall within the range reported in certain conditions, even below what has been described in more severe cases [6-14]. Hyperbilirubinemia is often a concern for newborns, due to the liver not having a full function at birth. In cases of infant homicide where blood traces are present, detection of elevated bilirubin levels in dried blood or serum could provide important presumptive information in the initial stages of the investigation. Future efforts may involve pilot studies evaluating samples from patients at various stages of the disease to expand the current findings.
Finally, the proposal that bilirubin in dried serum stains is photosensitive was verified in these studies, similar to what is known for bilirubin circulating in the bloodstream in vivo and in isolated serum samples. Thus, in cases where dried blood or serum has been exposed to direct sunlight, this method is not likely to be very useful. It was noted during these studies, however, that dried serum stains or dried blood drops containing elevated bilirubin could be exposed to indirect indoor (ceiling) lighting without any noticeable decline in UV fluorescence, even over several months.
In summary, the current study describes a simple, sensitive and nondestructive method for the detection of elevated bilirubin levels in blood serum.
- Fevery J. Bilirubin in clinical practice: a review. Liver Int. 2008 May;28(5):592-605. doi: 10.1111/j.1478-3231.2008.01716.x. PMID: 18433389.
- Fargo MV, Grogan SP, Saguil A. Evaluation of Jaundice in Adults. Am Fam Physician. 2017 Feb 1;95(3):164-168. PMID: 28145671.
- Muchowski KE. Evaluation and treatment of neonatal hyperbilirubinemia. Am Fam Physician. 2014 Jun 1;89(11):873-8. PMID: 25077393.
- Gondal B, Aronsohn A. A Systematic Approach to Patients with Jaundice. Semin Intervent Radiol. 2016 Dec;33(4):253-258. doi: 10.1055/s-0036-1592331. PMID: 27904243; PMCID: PMC5088098.
- Purohit T, Cappell MS. Primary biliary cirrhosis: Pathophysiology, clinical presentation and therapy. World J Hepatol. 2015 May 8;7(7):926-41. doi: 10.4254/wjh.v7.i7.926. PMID: 25954476; PMCID: PMC4419097.
- Kalakonda A, Jenkins BA, John S. Physiology, Bilirubin. [Updated 2021 Sep 16]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022. https://www.ncbi.nlm.nih.gov/books/NBK470290/
- Hossain MR, Pandey RK, Islam MF, Datar P, Gayam V, Puri P, Malar T. Acute Isolated Hyperbilirubinemia as a Presentation of Alcoholic Liver Disease: A Case Report and Literature Review. Case Reports Hepatol. 2018 Feb 12;2018:9403934. doi: 10.1155/2018/9403934. PMID: 29623226; PMCID: PMC5829357.
- Scharf C, Liebchen U, Paal M, Becker-Pennrich A, Irlbeck M, Zoller M, Schroeder I. Successful elimination of bilirubin in critically ill patients with acute liver dysfunction using a cytokine adsorber and albumin dialysis: a pilot study. Sci Rep. 2021 May 13;11(1):10190. doi: 10.1038/s41598-021-89712-4. PMID: 33986443; PMCID: PMC8119427.
- Souza MV, Novaes FS. Icterícia grave e miocardiopatia tireotóxica com trombo atrial [Serious jaundice and thyrotoxic myocardiopathy with atrial thrombus]. Arq Bras Endocrinol Metabol. 2012 Oct;56(7):456-60. Portuguese. doi: 10.1590/s0004-27302012000700008. PMID: 23108751.
- Ali H, Rizvi T, Niazi M, Galan M, Pyrsopoulos N. Autoimmune Hepatitis Induced after Treatment of Syphilitic Hepatitis. J Clin Transl Hepatol. 2022 Feb 28;10(1):174-177. doi: 10.14218/JCTH.2020.00178. Epub 2021 May 31. PMID: 35233387; PMCID: PMC8845154.
- Baig M, Zheng L, Farmer A. Severe Hyperbilirubinemia: A Rare Complication of Lyme Disease. Case Rep Gastrointest Med. 2019 Dec 24;2019:2762389. doi: 10.1155/2019/2762389. PMID: 31956450; PMCID: PMC6949660.
- Lin PMF, Chow SCY, Ng SWY, Ho AMH, Wan S. Acute liver failure with extreme hyperbilirubinemia secondary to endocarditis-related severe mitral and tricuspid regurgitation: a challenge and an opportunity for surgeons. J Thorac Dis. 2018 Feb;10(2):1067-1071. doi: 10.21037/jtd.2018.01.138. PMID: 29607182; PMCID: PMC5864625.
- Labori KJ, Raeder MG. Diagnostic approach to the patient with jaundice following trauma. Scand J Surg. 2004;93(3):176-83. doi: 10.1177/145749690409300302. PMID: 15544071.
- Cambou M, Greeley AM. Clinical Vignette: A case of autoimmune hepatitis. Proc UCLA Healthcare 2015; 19:1-3.
- Kearse KP. Ultraviolet 365 as an Alternative Light Source for Detection of Blood Serum. J Forensic Sci. 2020 Sep;65(5):1716-1721. doi: 10.1111/1556-4029.14439. Epub 2020 Apr 28. PMID: 32343369; PMCID: PMC7496641.
- Kearse KP. Environmental influence on blood serum detection using ultraviolet 365. J. Forensic Sci Res. 2021; 5: 130-036. doi: 10.29328/journal.jfsr.1001024
- Kearse KP. The reddish color of bloodstains on the Shroud of Turin: investigation of two hypotheses. J His Arch & Anthropol Sci. 2020; 5:101‒107. DOI: 10.15406/jhaas.2020.05.00223