Case Report
Enclosure asphyxia as a cause of death in 3 Nigerian children trapped at the boot of car-Case reports and review of literature

Martin A Nzegwu 1*, FMCPath Nig2, DB Olusina Francis Ikechukwu Ukekwe2 and Victor Nzegwu2
1Professor and Clinical Dean University of Nigeria Medical School, Nigeria
2Department of Morbid Anatomy, University of Nigeria Medical School, Nigeria
*Address for Correspondence: Dr. Martin A Nzegwu, Associate Professor and Clinical Dean University of Nigeria Medical School, Ituku Ozalla UNTH Enugu, Nigeria, Tel: +2348055509566; Email: [email protected]
Dates: Submitted: 26 September 2017; Approved: 10 October 2017; Published: 11 October 2017
How to cite this article: Nzegwu MA, Path Nig FMC, Ikechukwu Ukekwe DBOF, Nzegwu V. Enclosure asphyxia as a cause of death in 3 Nigerian children trapped at the boot of car-Case reports and review of literature. J Forensic Sci Res. 2017; 1: 087-091.
DOI: 10.29328/journal.jfsr.1001010
Copyright License: © 2017 Nzegwu NA, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Enclosure asphyxia; Nigerian children; Cause of death
Abstract
The paper reviews enclosure asphyxia as a cause of death of three Nigerian children aged three years, five years and seven years respectively, who were found dead and locked in the boot of a Mercedes Benz 200E Sedan car a day after they were declared missing. The first two were siblings of the same parent whose fathers actually owned the car, while the older child was a neighbour kid all of whom were well known to each other as friends and playmates. They had gone missing for a few hours prior to being seen playing together. Search parties were raised and they were never found until the following day when they were found dead in the boot of the car parked a few meters away from the house under a tree. Incidentally the same car was driven round the neighbourhood for 3 hours during the search the previous day with no inkling that they were in the boot of the car. Autopsy was ordered by the coroner to determine the cause of death.
Introduction
Enclosure asphyxia is relatively rare in literature as a cause of death. It has been described in industrialized countries as the type of asphyxiation which occurs in confined spaces, such as process vessels, cryogenic enclosures, pump and expander enclosures/ducts, totally enclosed working areas and pits and in most cases result from ignorance of properties of nitrogen and inert gases [1].
There are almost no reported cases in Children especially in a developing country setting as in Nigeria where it has occurred in an unexpected place like the boot of a car from unbridled desire of the average child to explore his environment. The possibility of its occurrence in this setting more so when the car in question was driven for close to three hour in search of these children in the neighbourhood, thus raising the carbon monoxide levels, raises fresh perspectives on child education in homes and schools to enlightening children and parents of the possibility of such entrapment and the need to avoid exploring enclosures. The diagnosis was of enclosure asphyxia was made from the autopsy finding of classical signs of asphyxia at autopsy in the absence of either trauma or signs of strangulation, or maceration with an ambient temperature of between 13-24oC. The hyoid bone of all these children was intact and normal.
Results
Full body autopsy was carried out on the bodies of the kids, all of whom were males aged 3, 5 and 7. See figures 1A-C, showing all male children of Negroid descent in playing clothes bleeding from the nasal and buccal orifices without any obvious external signs of violence except for minor bruises on the external surfaces and forehead apparently from failed attempts to forcibly open the boot from within.
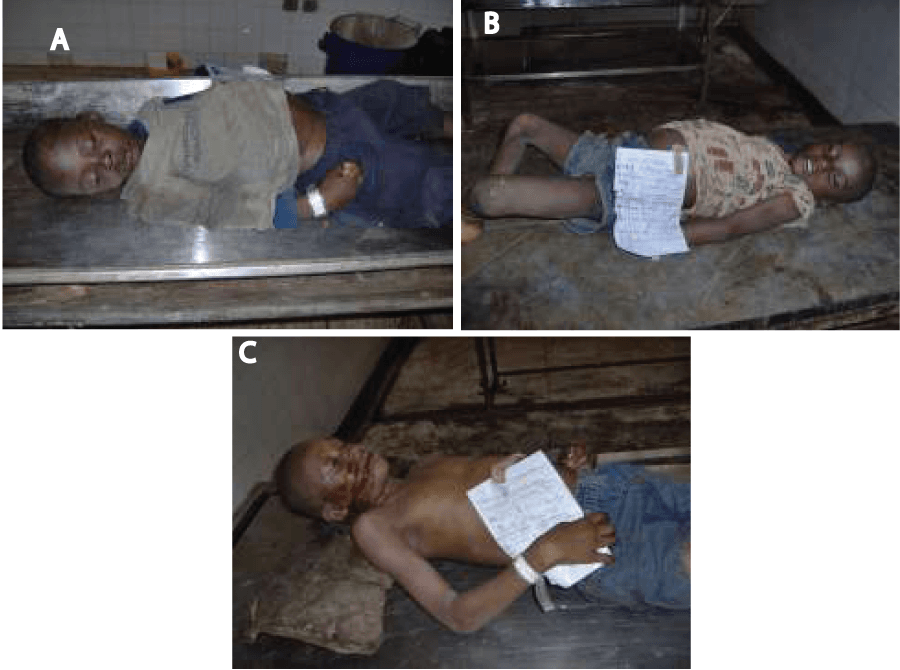
Figure 1A-C: Shows the bodies of all three kids before autopsy aged 3, 5 and 7 respectively.
Case 1
On the autopsy table is the body of a three year old male whose size is appropriate for age and without external signs of strangulation or violence. There is mild spontaneous bleeding from the nasal and oral orifices and the presence of central cyanosis with a bluish tinge on the tongue. On opening up the hyoid bone is intact and normal. The lungs were enlarged bilaterally and had a purplish hue to its colour (cyanosis) with patched of sub-pleural haemorrhages and intra parenchymal haemorrhages.
There is also marked fluidity of blood with absence of clots in the entire cardiovascular system. The right side of the heart was dilated in keeping with respiratory failure. There were also sub pericardial haemorrhages and the cerebral cortex was oedematous with flattening of the gyri and obliteration of the sulci. There are also meningeal and subarachnoid haemorrhages. The cause of death was diagnosed as enclosure Asphyxia with respiratory Failure.
Case 2
The body of a five year old male whose size is appropriate for age and without external signs of strangulation or violence. There is mild spontaneous bleeding from the nasal and oral orifices. On opening up the hyoid bone is intact and normal. The lungs were enlarged bilaterally and had a purplish hue to its colour (cyanosis) with patched of sub-pleural haemorrhages and intra parenchymal haemorrhages.
There is also marked fluidity of blood with absence of clots in the entire cardiovascular system. The right side of the heart was dilated in keeping with respiratory failure. There were also sub pericardial haemorrhages and the cerebral cortex was oedematous with meningeal and subarachnoid haemorrhages. The cause of death was diagnosed as enclosure Asphyxia with respiratory Failure.
Case 3
On the autopsy table is the body of a seven year old male whose size is appropriate for age and without external signs of strangulation or violence. There is marked conjuctival suffusion bilaterally with marked spontaneous bleeding from the nasal and oral orifices and the presence of central cyanosis with a bluish tinge on the tongue. On opening up the hyoid bone is intact and normal. The lungs were enlarged bilaterally and had a purplish hue to its colour (cyanosis) with patched of sub-pleural haemorrhages and intra parenchymal haemorrhages.
There is also marked fluidity of blood with absence of clots in the entire system. The right side of the heart was dilated in keeping with respiratory failure. There were also sub pericardial haemorrhages and the cerebral cortex was oedematous with flattening of the gyri and obliteration of the sulci. There is also meningeal and subarachnoid haemorrhages. The cause of death was diagnosed as enclosure Asphyxia with respiratory Failure (Figures 2,3).

Figure 2: Shows marked conjunctival suffusion and evidence of spontaneous bleeding from the nasal and buccal cavities.

Figure 3: Shows the dilated right ventricle without any blood clots. Note the fluidity of blood with areas of sub pleural haemorrhages.
All lungs histology was consistent with adult respiratory distress with hyaline membrane changes and diffuse alveolar damage while the kidneys showed acute tubular necrosis (Figure 4a,b).
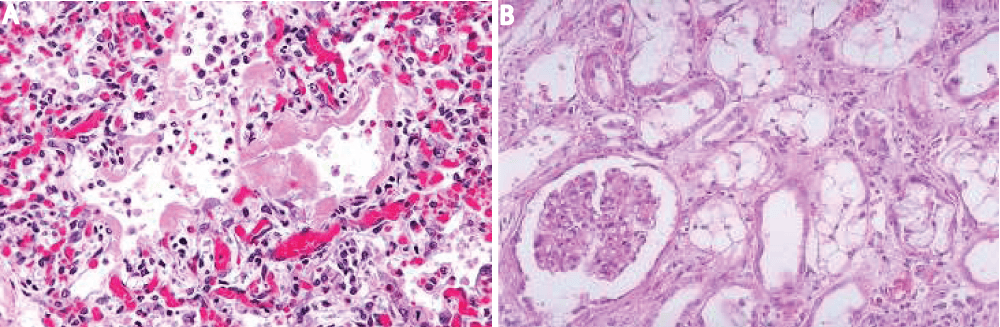
Figure 4: A: Diffuse Alveolar damage. B: Acute tubular necrosis.
Discussion
These three kids who were neighbours were last seen playing together within their compound or premises when they suddenly seemingly disappeared. The interval between the times their bodies were found at 0900hours the next day and when they were declared missing a day prior was roughly 21 hours. Their bodies was found by the father of the first two siblings when he was about to wash his car while opening the boot for an unrelated issue reason of retrieving his cleaning rag. He is a law enforcement officer. The ambient temperature about this time and season in Nigeria was averaging a high of 24oC and a low of 13oC in Enugu, Nigeria in the heart of the hamarttan season equivalent to the winter period in the west. There unique thing in this scenario is that these kids were not known to have any prior affinity for fondling with cars. They were all found dead with no signs of life. The boot may not have been overtly air tight but the same car was driven around the neighbourhood to search for these kids for close to three hours the same night without any inkling that they may have been in the boot. Apparently they were already dead or comatose by then. An air tight study was not conducted but with the size relative to the oxygen demand for three active children it seems most plausible that relative hypoxia was the cause of death.
Klaus et al., reported “There are almost as many different possibilities of grouping asphyxia as there are authors, and there are different definitions of the asphyxia itself” [2]. One possibility is to define asphyxia, all-encompassingly, as the failure of the body cells to either receive or utilize oxygen; more or less in parallel with an increase in the blood carbon dioxide level [2]. This led to the differentiation between external or enclosure asphyxia and internal asphyxia [2]. The former is what we are dealing with in this literature.
When an individual is in an enclosed space or compartment the concentration of oxygen therein continually falls, Concentration, thinking and decision making are impaired when the oxygen concentration falls slightly below this norm [3], these effects are also not noticeable to the affected individual [3]. The normal oxygen concentration in the air is approximately 21%. If this oxygen concentration falls only slightly or the concentration of other gases increase a situation is rapidly reached where the risks of asphyxia are significant [4].
It is therefore clear that within minutes after these kids were trapped they would have been alarmed almost immediately and struggled to get out thereby depleting the amount of oxygen in the enclosure while considerable increasing the concentration of carbondioxide rapidly resulting in asphyxia within possible 30 minutes of the whole episode. The driving around of the vehicle with the children in the boot for about three hours obviously further increased the carbon dioxide levels and possibly introduced carbon monoxide further worsening the asphyxia. If these children were already unconscious in the best case senerio they would surely have all passed on with this development.
The underlying pathophysiological mechanism in asphyxia related deaths is the lack of oxygen. Thus it is justified to some extent to talk of about a common reaction pattern. This relates to the agonal process as well as autopsy findings [2].
For more than 100 years, the diagnosis of asphyxia has been based upon the classical vital signs of asphyxia. Ollivier [5], described a finding in autopsy of persons who had been trampled by crowds, with craniocervical cyanosis, subconjunctival haemorrhage, and cerebral vascular engorgement. He then applied the term masque ecchymotic to desribe these features. Similar reports subsequently appeared in the French and German literature, [6-8] but without explanation. In 1900, Perthes [7], observed mental dullness, hyperpyrexia, hemoptysis, tachypnea, and contusion pneumonia and since then, petechial hemorrhages of the mucus membranes, epistaxis, hematemesis, rectal bleeding, hematoma of the esophagus, albuminuria, microscopic hematuria, paraplegia, peripheral nerve damage, amnesia, and convulsions have been described in what is now known as traumatic asphyxia in literature [9-15].
The common symptoms in all these deaths are complete absence of external forces of violence except for few bruises on the fore arms of the 7 year old and 5 year old presumed to be sustained in an attempt to forcible open the boot. Other important negatives are the normal hyoid bone and absence of neck haemorrhages which are all in keeping with death without strangulation. The positives findings in agreement with asphyxia include sub-serous intra thoracic haemorrhages especially affecting the sub pleural spaces and the sub-pericardial spaces. These signs are in keeping with reports from Kratter [16], Roderer [17] and Liman [18]. Liman indeed reported that “subserous ecchymoses, namely of thoracic organs, can be a valuable symptom of an asphyxial death, but their absence do not an asphyxial death nor do they in any way allow to distinguish between self infliction and infliction by another person” [18]. In the lungs focal haemorrhagic odema was seen in all the lungs examined with the intraparenchymal haemorrhage grossly viscible in all the lungs examined. The finding has also been documented by many authors including von Hoffmann [19], Lochte [20]. In conclusion we say that enclosure asphyxia which although is more common in the industrialized nations can also be found here especially in children who find it intriguing to explore enclosures and areas of entrapment such as the boot of a car.
References
- Puschel K, Turk E, Lach H. Asphyxia related deaths. Foren Sci Int. 2004; 144: 211-214. Ref.: https://goo.gl/hnCJQJ
- http://www.eiga.eu cited on 10-04-2012.
- www.eiga.org/index.php? Cited on the 10-04-2012.
- www.linde-gas.com.ph/...campaign_Cited on the 10-03-2012.
- Ollivier DA. Medical relationship of the events that occurred in the Champ-de-Mars on June 14, 1837. Ann. hygiene. 1837; 18: 485.
- Hueter C. Ueber die Dilatation der Blutgefaesse der Kopfes bei schweren Verletzungen des Unterleibes. Deutsche Ztschr. f. Chir. 1874; 4: 382.
- Perthes G. Ueber "Druckstauung”. Deutsche Ztschr F Chir Lv. 1900; 384.
- Tardieu A. Memoire sur la mort par suffocation. Ann. d'hyg. 1855; 4:371.
- Gardner EK. Traumatic Asphyxia. Brit Med J. 1941; 2: 545.
- Gordon WI, Thomson AMW. Traumatic Asphyxia: With Illustrating Cases. Glasgow Med J. 1938; 130: 180. Ref.: https://goo.gl/Efh3Hq
- Green TM. Traumatic Asphyxia. Surg Gynec. Obstet. 1922; 35: 129.
- Hamilton JB. Note on Traumatic Asphyxia with Ocular Complications. Brit J Ophth. 1930; 14: 22.
- Pierce FE. Traumatic Asphyxia with Report of two Cases. Q Bull Northwest Univ Med Sch. 1910; 12: 39-44. Ref.: https://goo.gl/pH9MTv
- Stickney JM, Hagedorn AB. Chest Injuries and Traumatic Asphyxia. Proc Mayo Clin. 1944; 19: 207.
- Winslow R. A Case of So-Called Traumatic Asphyxia. Med News of N Y. 1905; 86: 207.
- Kratter J. Wien Klin Wchnschr.1894; 379.
- Roderer JG. 1760 De submerisis aut suffocates. Gottingen.
- www.medicinaforense.cl/sw.a/00000994 Cited on 11042012.
- Von Hoffmann C. Cal State J Med. 1910; 8: 216.
- Lochte T. DTSCH z Gesamte Gerichtl Med. 1948.